CASE STUDY
CASE STUDY: VASCULAR OCCLUSION
Dr Hayder Ria, medical lead for Harley Street Dermal, treats a vascular occulusion on a male patient in this case study
PATIENT OVERVIEW
Gender: male
Age: 45
Presenting complaint: vascular occlusion on the chin
Intervention: hyaluronidase, medication & hyperbaric oxygen
Practitioner: Dr Hayder Ria
DR HAYDER RIA
Dr Hayder Ria is an experienced cosmetic injector with over 10 years experience. He is the medical lead for Harley Street Dermal, a leading cosmetic clinic in London. He remains a clinical lead within the NHS and is a member of the Royal College of General Practitioners (RCGP).
Although extremely rare, vascular occlusions are one of the most serious complications in aesthetics, and recognising them quickly is crucial.
A vascular occlusion occurs when dermal filler is injected into an artery, causing it to be obstructed and potentially leading to necrosis to tissues supplied by the artery. While these occurrences are rare (around one in 10,000), delays with management and lack of confidence can negatively affect patient outcomes. This case demonstrates how swift recognition and systematic intervention can help achieve positive outcomes, even in complex situations.

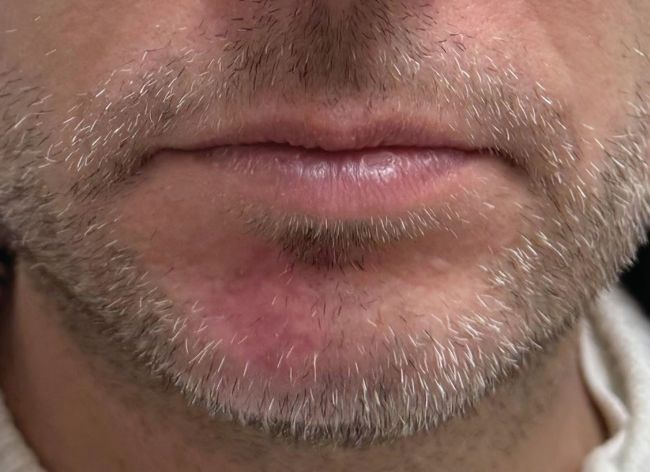
Three days post-treatment (how the patient presented)
CASE STUDY
In this case, the patient (SA) presented to the clinic after having had chin injections with hyaluronic acid dermal filler to enhance the structure of their chin. The treatment was performed elsewhere. They contacted the clinic three days after having had their treatment because they developed increasing soreness and weeping around the injection site. The patient immediately came to the clinic upon our request, and their chin looked like the picture above. This was immediately recognised as the third stage of a vascular occlusion (bacterial bioburden). The injected area was weeping and SA was in pain. There was poor capillary refill around the right side of the chin as well as the mucosal tissue around the lower gums on the same side. SA was given immediate treatment which included:
• High dose dissolving (1ml hyaluronidase, 1500IU diluted in 1ml of 0.9% bacteriostatic saline) – using microcannula (25G) to flood the area along with firm compression and massage
• High dose aspirin (300mg for seven days)
• High dose oral steroid (Prednisolone 40mg for five days- with gastric cover using Omeprazole Gastro-resistant capsules 20mg)
SA was advised that he would need daily reviews for the first week and would need to apply a warm compress for five to 10 minutes several times a day to increase the chances of breaking down the dermal filler and improving perfusion into the tissues. He was also booked for five sessions of hyperbaric oxygen treatment (90 minute sessions) to maximise oxygenation to the tissues. SA was seen again the next day and given another 1ml of high dose dissolving. The local NHS plastics department was also informed just in case further intervention was required.

Day 5 post-treatment (early progress – “worse before better”)
By day 5, the treatment area looked darker as the outermost layers of tissue began to coagulate and slough off, giving the appearance of necrosis which can often make practitioners concerned that the patient’s condition is getting worse. Experienced practitioners will know that this is part of the recovery process and that things will often look worse before they look better. Despite the seemingly worse-looking appearance, capillary refill of the surrounding tissues and the lower gums was now less than three seconds; a promising sign of recovery. Reviews were now reduced to every few days as things continued to improve.

Day 14 post-treatment (recovery phase)
Two weeks later, the tissues looked much improved with only mild redness remaining as the tissues continued to heal. The patient raised concern that his beard had not yet begun to regrow in the affected area and was worried that he would require topical hypertrichotic treatments (such as minoxidil) or even a hair transplant. He was reassured that because the occlusion was managed quickly, follicular damage was unlikely to be permanent – and indeed, hair regrowth later confirmed this.
One month post treatment
By one month post treatment, the patient had made a near-full recovery, with no significant scarring or textural changes. The case demonstrated how even a serious complication can resolve favourably when treated promptly and consistently.
CONCLUSION
This case serves as a valuable reminder that while vascular occlusions are rare, they can happen in any clinical setting. With rapid recognition, immediate access to dissolving agents, and structured follow-up, patients can make a full recovery. At Harley Street Dermal, our focus remains on excellence in aesthetic outcomes underpinned by patient safety, education, and evidence-based care.
KEY POINTS TO CONSIDER:
• Act fast
The most important thing to do when managing a vascular occlusion is to respond quickly and thoroughly.
• Hyaluronidase diffuses
Many injectors think that because the artery is blocked (in this case, the ascending mental artery) that the dissolving needs to be injected directly into the artery. This would be extremely difficult as the median artery width is around 0.7mm, meaning pinpoint precision under ultrasound, which isn’t practical in an emergency setting. Hyaluronidase tends to diffuse across the tissues meaning that it can enter the artery as long as it’s injected close by in high concentrations
• Things will look worse before they look better
"The night is often darkest just before the dawn." Reassure your patient that in cases such as these, things will look worse before they look better
• Don’t delay, defer
Don’t be afraid to escalate the case to your local NHS plastics service if you feel out of your depth.