MALE AGA
Male ANDROGENETIC ALOPECIA
Dr Xavier Goodarzian and Luis Alexandre Costa describe the consultation and approach to treatment
Over the past decade there has been an increase in demand for hair regrowth treatments. Androgenic alopecia (AGA) is one of the main causes of hair loss and accounts for 80% of the patients we see in our hair clinic.
Individuals who seek professional assistance for hair regrowth treatments usually present at an early stage. Although we have met patients with AGA at an advanced stage with unrealistic expectations, most of our patients are at a point where nonsurgical hair treatments can have a beneficial impact. The motivations of the consultation and psychological history are crucial not only to understand the patient, but also from a legal and ethical point of view, as many have unrealistic expectations and think high prices guarantee results.
MALE AGA
Male AGA is a genetic condition characterised as persistent, progressive and patterned hair thinning and loss primarily at the crown and temples in the scalp. It is the most common cause of hair loss and a common cosmetic complaint, perceived as a condition with significant emotional impact.1 In AGA, hair follicles become increasingly sensitive to androgens over time. The metabolite of the testosterone, dihydrotestosterone (DHT) has a direct impact in its development.2 As DHT accumulates in androgen-sensitive AGA tissues, the AGA-prone hair follicles become sensitive to DHT and start to diminish in size, resulting in hair thinning and eventually AGA.3
CONSULTATION
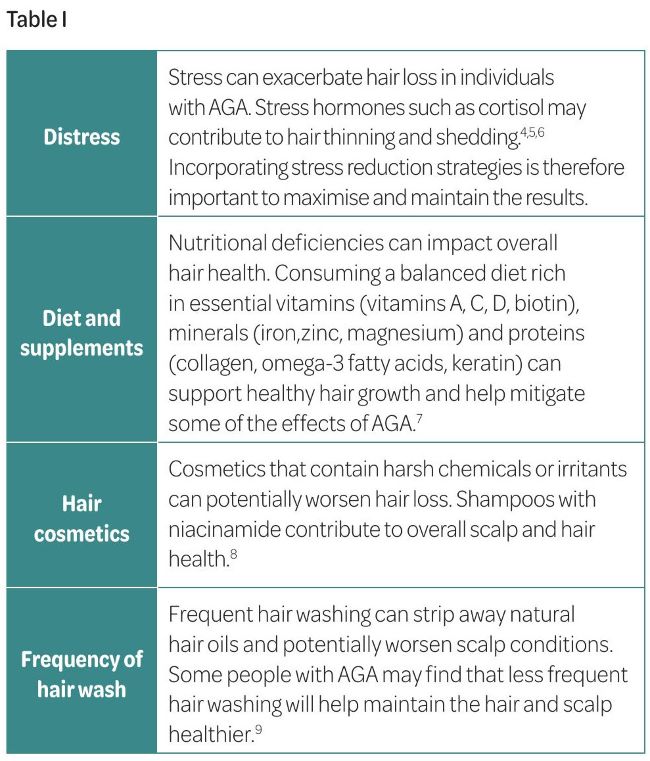
In the consultation, it is essential to examine the scalp and the hair as well as identifying factors that could be inducing alopecia. Distress, diet, hair cosmetics, frequency of hair wash are important factors to consider when obtaining the history of the present complaint. Table I summarises the impact of these factors on male AGA.

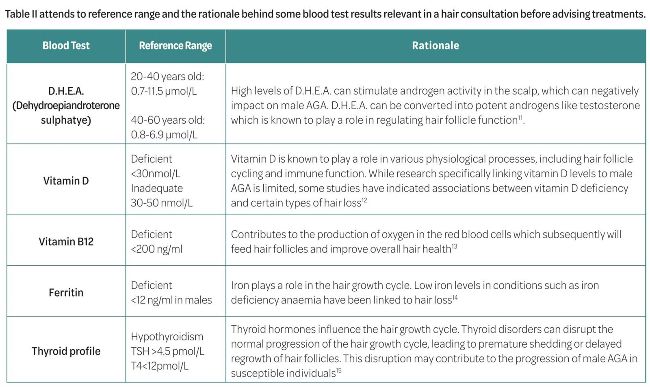
While male AGA is primarily attributed to genetic and hormonal factors, a blood tests can be helpful to understand the underlying causes or exacerbating factors. Specific blood tests include hormone profile, thyroid function, D.H.E.A., vitamin D, vitamin B12 and iron levels. The hormone profile blood test is important and may be particularly relevant in a young male with AGA. Androgenic effects of testosterone have a direct impact on hair loss but with an abnormal hormone profile these can be intensified, and the dihydrotestosterone (DHT) can produce progressively weaker hair due to the follicles’ failure to thrive.10 Additionally, estrogen, can influence hair growth patterns and increase the amount of time hair spends in the growing phase (anagen), leading to thicker and stronger hair, so when levels are decreased the hair may become susceptible to thinning.
In male AGA, it is also important to explore the use of anabolic steroids in the medical history as it may negatively impact the condition. Anabolic steroids are thought to be linked to increase production of DHT.16 If this is the case, practitioners should recommend discontinuing the use of anabolic steroids before initiating any treatments.
TREATMENTS FOR MALE AGA
Platelet-rich plasma and platelet-rich fibrin
Platelet-rich plasma (PRP) is an autologous concentration of human platelets, obtained from a small volume of plasma.17 It contains a combination of protein growth factors (GF) chemokines, cytokines and three proteins in the blood (fibrin, fibronectin and vitronectin) known to act as biological adhesive material. The significance behind its use relates to enhancement of the rate and quality of the healing process by promoting cell proliferation, angiogenesis and collagen production.18,19,20 The complete process includes collecting blood which is to be centrifuged to provide the platelet concentrate.21 In some cases, the PRP may be activated using calcium chloride (CaCl2) or another activating agent (calcium gluconate, Thrombin) to release GF from the platelets, enhancing its regenerative capabilities. A study by Cavallo et al. (2016) concluded that the activation modality will influence the release kinetics of GF and that the selection of PRP activation strategies should consider not only the type of procedure but also the intended biological outcomes.17 CaCl2 exhibited a gradual release pattern over time, starting with a lower initial level and gradually increasing the release of GF. This trend resulted in similar or even higher levels of growth factors at the 24-hour evaluation point. GFs have a short half-life (from minutes to hours) and, if not used promptly upon release, they risk degradation before additional tissue receptors become accessible.17 From a clinical perspective, this aspect may be one of the causes related to poor results reported by aesthetic practitioners. PRP is then injected sub or intradermally into the desired areas.
A meta-analysis on the evidence of PRP for AGA by Giordano et al (2018)18 identified insufficient evidence on the efficacy of the PRP to treat AGA. The results were satisfactory as most of the participants had a significant increased number of hairs by cm2 and increase in hair cross-section thickness at three months, but the included studies had a small total number of patients. There were also no standard methods of PRP preparation and activation highlighted in the methods, which compromises the homogeneity of the product composition in between the studies.18
Platelet-rich fibrin (PRF) involves a slightly different preparation method which rely on simpler centrifugation process.21 After blood is drawn, it is centrifuged without anticoagulants, resulting in the formation of a fibrin clot containing platelets and other blood components. PRF is considered to have a more complex and threedimensional structure compared to PRP. PRF generally yields lower platelet concentrations compared to PRP but may contain a higher concentration of leukocytes and growth factors due to its fibrin matrix. When compared to PRP, PRF has a slower release profile, with growth factors gradually being released over a longer period.21 Several studies have explored the use of PRP and PRF in the treatment of male AGA with varying results. Some studies support PRP and some support PRF with regards to improved hair thickness, density and overall regrowth. Ultimately, the choice between PRP and PRF should depend on factors such as patient preferences, clinician experience and specific individual characteristics of the patient.
Polynucleotides
Polynucleotides (PN) have recently become very popular in the treatment of skin ageing and hair loss. Even though PN have been around for many decades, the use of PN has mostly taken off over the last two to three years. PN are chains of nucleotides, which are essentially basic fragments of DNA. When multiple nucleotides link together, they form a chain comprised of single nucleotide units. When these chains are short, they are called polydeoxyribonucleotides (PDRN). When the chains are longer, these are named PN. PDRN have been used as a prescription medicine for many years in Europe for tissue repair, including bone, cartilage, tendons, muscle and wounds (epithelial tissue). The more recent PNs, are in fact considered medical devices and not prescription drugs. The DNA used for current PN is derived from fish (salmon or trout), more specifically their gonads. Once the DNA is extracted, it is purified and sterilised to ensure there is no protein or lipid contamination from the animal source in the product.22
PN work by increasing fibroblast activity, resulting in increased collagen, elastin and hyaluronic acid in the tissues.22,23 These mechanism of action supports the use of PN for skin rejuvenation, for treatment of sun damage and pigmentation. PN also shorten the healing phase reducing the downtime following procedures.26 The action on fibroblasts leading to enhancement of the skin and increased blood flow also positively benefits the hair follicles in cases of male AGA. A 2014 study24 from the university of Pisa showed that the use of Plinest Hair (a PN product specifically designed for scalp and hair) significantly improved the density of hair and the thickness of hair. In the study, the use of PN demonstrated a reduction of hair loss when manipulating the hair (hair pull test) and washing. In the study, a trichogram analysis confirmed reduction of the telogen phase and an increase in the anagen phase.
PN should be performed as a course of treatments. For the skin, PN should be administered in a course of three to four sessions, whereas for male AGA, a minimum of eight sessions is often recommended. This treatment can also be combined with other treatments. It is considered a treatment simple to administer with virtually no negative side-effects.
Minoxidil
Minoxidil is the most popular topical agent used in AGA due to his low cost, safety and availability over the counter. It has been approved for use in men and women and is available in 2% or 5% formulations. It’s a potassium channel opener, known to hyperpolarise the cell membrane and increase blood flow. It plays a role in stimulating hair follicles cells to proliferate and decrease the miniaturisation of follicles, promoting regrowth. While vasodilation may contribute to the overall efficacy of minoxidil in promoting hair growth, it is not the sole mechanism of action. The exact way minoxidil works to stimulate hair growth is still not completely understood, and further research is ongoing in this area. The British National Formulary (BNF)25 recommends applying 0.5 capful twice a day for extra strength foam and 1ml twice daily extra strength solution to the affected areas on the scalp with the instructions to discontinue if no clinical improvement seen after 16 weeks (foam) or one year (solution).
New research supports the use of oral minoxidil in the form of a 2.5 mg tablet. A study26 found that low dose of 2.5 mg/day oral minoxidil led to significant improvement in hair density and hair thickness in males with AGA. Another multicentre study27 concluded that low dose minoxidil resulted in significant improvements in hair density and hair count in most participants, however some experience side-effects such as hypotension and hypertrichosis.
Before prescribing oral minoxidil we recommend a baseline assessment, including a blood pressure to establish a reference point for monitoring during the treatment, followed by regular blood pressure monitoring through the treatment as hypotension is a potential side-effect. Start with a low dose of oral minoxidil and titrate gradually based on individual response and tolerance. Avoid abrupt dosage changes to minimise the risk of adverse effects; and educate your patients about other common side-effects of this pharmacotherapy such as ankle swelling and hypertrichosis.
Finasteride
Finasteride is a 5-alpha-reductase inhibitor and blocks the conversion of testosterone to DHT. It promotes hair regrowth and prevents further hair loss in a significant proportion of men with AGA.28 Several studies also associated AGA progression with age. Researchers believe that the younger patient is, more the likelihood of improvement when compared to older men. The BNF25 recommends finasteride 1mg, once a day to treat male AGA, with continuous use for three to six months. Before prescribing finasteride, it is important to always discuss common side-effects, like sexual dysfunction, breast anomalies and skin reactions. The overall incidence of sexual function disorders such as decreased libido, ejaculation issues and erectile dysfunction are known to be significantly greater in men taking finasteride29 but all sexual adverse events are usually reversed on discontinuing pharmacotherapy.
Microneedling
Microneedling (MN) is a treatment that induces the wound healing cascade with minimal damage to the stratum corneum using needles. It induces collagen formation, creation of new blood vessels and growth factor production in treated areas.30 It is a treatment that has shown promising results treating AGA when combined with topical minoxidil. Arandomised blinded study of the effects of the micro needling in AGA confirmed that a group treated with MN along with minoxidil had more than 50% of improvement and was statistically superior to the group just treated with topical minoxidil alone (only 4% improvement).28
The results of this study are satisfactory with all men from the micro needling group reporting a sustainable response after eight months. The countersense is that all men included in the study were on finasteride which can compromise the reliability of the efficacy of the MN as well as the lack of specification regarding the different sizes of the needles used, and the frequency and end point of the procedure which are also not in detail.
Personalising the treatment - pharmacogenomics
Pharmacogenomics explores how an individual genetic makeup influences their responses to medications.31 In our clinics, we have the opportunity of providing efficient and personalised treatment plans after identifying the patient’s genetic variations that will affect drug efficacy and metabolism by analysing their genetic profile. The use of pharmacogenomics allows us to prescribe treatment plans that are more likely to be effective and well-tolerated based on the patient’s genetic makeup and their individual needs. In addition, pharmacogenomics also helps predicting the likelihood of treatment response allowing informed decisions to optimise treatment outcomes.31
SUMMARY
Treating male androgenetic alopecia involves a range of options. Each treatment has its benefits and considerations, and the choice should be tailored to individual patient needs. Patient preferences, clinician experience, and specific characteristics of the patient, including socialpsychological factors, should be considered. Pharmacogenomics can provide insights into medication efficacy and adverse effects, guiding treatment selection, however, the success of therapy is multifactorial as it will also depend on managing stress, adjusting hormonal changes, and lifestyle modifications. Stress management techniques, addressing hormonal imbalances, and lifestyle advice such as a balanced diet and regular exercise can complement treatment efficacy. A holistic approach, considering both medical interventions and lifestyle factors, is crucial for optimising treatment outcomes in male androgenetic alopecia.
Case study:
Male, 31 years old, healthy with no past medical history.
• Diagnosis: male AGA
• Blood test results: normal
• Pharmacogenomics: finasteride (86%) and minoxidil (73%) suitability based on genetic profile
Personalised treatment plan
• Prescribed medicines: finasteride 1mg once a day; minoxidil 2.5 mg once a day
• Platelet-rich plasma (three sessions – four to five weeks apart)
• Polynucleotides (eight sessions – four weeks apart)

Before Jan 2023

After Jan 2024
The platelet-rich plasma and the polynucleotides were administered with a minimum of a two-week interval.
REFERENCES
1. English Jr RS. A hypothetical pathogenesis model for androgenic alopecia: clarifying the dihydrotestosterone paradox and ratelimiting recovery factors. Medical hypothesis (2018). 111:73-81
2. Lolli D, Pallotti F, Rossi A. Androgenic Alopecia: a review. Endocrine (2017). 57: 9-17.
3. Yang YC, Fu HC, Wu CY, Wei KT, Huang KE, Kang HY. Androgen receptor accelerates premature senescence of human dermal papilla cells in association with DNA damage. PLos One (2013).
4. Dinh, Q.Q., R. Sinclair, Female pattern hair loss: current treatment concepts. Clin Interv Aging, 2007. 2(2): 189-99.
5. Shin, H., et al., Acute Stress-Induced Changes in Follicular Dermal Papilla Cells and Mobilization of Mast Cells: Implications for Hair Growth. Ann Dermatol, 2016. 28(5): 600-606.
6. Thom, E., Stress and the Hair Growth Cycle: Cortisol-Induced Hair Growth Disruption. J Drugs. Dermatol, 2016. 15(8): 1001-4.
7. Glynis, A., A Double-Blind, Placebo-Controlled Study Evaluating the Efficacy of an Oral Supplement in Women with SelfPerceived Thinning Hair. The Journal of Clinical and Aesthetic Dermatology, 2012. 5(11): 28-34.
8. Choi, Y.H., Shin, J.Y., Kim, J., Kang, N.G., & Lee, S. Niacinamide Down-Regulates the Expression of DKK-1 and Protects Cells from Oxidative Stress in Cultured Human Dermal Papilla Cells. Clin Cosmet Investig Dermatol, 2021. Oct 18;14:1519-1528. doi: 10.2147/CCID.S334145. PMID: 34703266; PMCID: PMC8536842.
9. Sinclair, R. Dandruff and seborrheic dermatitis: a head scratcher. The Australasian Journal of Dermatology, 2016.
10. Ramos, P.M. and H.A. Miot, Female Pattern Hair Loss: a clinical and pathophysiological review. An Bras Dermatol, 2015. 90(4): 529-43.
11. Arck, P.C., Handjiski, B., Hagen, E., et al. Is there a ‘gut-brain-skin axis’? Experimental Dermatology, 2010. 19(5): 401-405.
12. Amor KT, Rashid M, Mirmirani P. Does D matter? The role of Vitamin D in hair disorders and hair follicle cycling. Dermatol Online J. 2010 Feb 15:16 (2):3.
13. Rushton DH, Norris MJ, Busuttil N. Causes of hair loss and the developments in hair rejuvenation. Int J Cosmet Sci. 2002 Feb; 24 (1): 17-23.
14. Salinas M, Leiva-Salinas M, Flores E, Lopez GArrigos M, LeivaSalinas C. Alopecia and Iron Deficiency: An interventional Pilot Study in Primary Care to Improve the Request of Ferritin. Adv Hematol. 2020.
15. Contreras-Jurado, C., et al., Thyroid hormone signaling controls hair follicle stem cell function. Mol Biol Cell, 2015. 26(7): 1263-72.
16. Kaufman, K.D., Androgens and alopecia. Mol Cell Endocrinol, 1998. 146(1-2): 61-8Author: Kaufman KD Year: 1998.
17. Cavallo, C., et al., Platelet-Rich Plasma: The Choice of Activation Method Affects the Release of Bioactive Molecules. Biomed Res Int, 2016. 2016: 6591717.
18. Giordano S, Romeo M, Di Summa P, Salval A, Lankinen P. A Metaanalysis on Evidence of Platelet-Rich Plasma for Androgenic Alopecia, 2018.
19. Kevy S, Jacobson M. Preparation of growth factors enriched autologous platelet gel. Poceedings of the 27th Annual Meeting of Service Biomaterials. April 2001.
20. Marx RE, Carlson ER, Eichstaedt R. Platelet Rich Plasma: Growth factor enhancement for bone grafts. Oral Surgery 85:638, 1998.
21. Choukroun J, Adda F, Schoeffler C, Vervelle A. [An opportunity in perio-implantology: the PRF]. Implantodontie 2001;42:55-62.
22. Cavallini M, Bartoletti E, Maioli L, Massirone A, Palmieri IP, Papagni M, Priori M, Trocchi G, members of The Polynucleotides HPT Priming Board, Collegio Italiano delle Società Scientifiche di Medicina Estetica (Italian College of the Aesthetic Medicine Scientific Societies) -SIME, AGORÀ, SIES. Consensus Report on the Use of PN-HPT (Polynucleotides Highly Purified Technology) in Aesthetic Medicine. Journal of Cosmetic Dermatology. 2020;1-7.
23. Cavallini, Papagni. Polynucleotides HPT at the hair follicle level. Aesthetic Medicine. April-June 2021;7(2).
24. Gianfaldoni R, Gianfaldoni S, Nannipieri A, Lotti T. A polynucleotide–based product to treat female hormonal hair loss. Prime. July/August 2014;30-36.
25. Joint Formulary Committee. British National Formulary. London: BMJ group and pharmaceutical press, 2024.
26. Situm, M., Bulat, V., Lugović-Mihić, L., et al., Efficacy and Safety of Low-Dose Oral Minoxidil in Male Androgenetic Alopecia. Acta Dermatovenerol Croat, 27(3), 140-144, October 2019.
27. Fertig, R.M., Gamret, A.C., Darwin, E., et al., Oral Minoxidil in Androgenetic Alopecia: A Retrospective, Multicenter Study in 62 Patients. JAm Acad Dermatol. 2018 Nov;79(5):AB204.
28. Sonnenreich P, Dunkin MA. Treating Androgenic Alopecia: A Review of Medical Treatments. The Dermatologist, 2020 Volume 28 – Issue 12
29. McClellan KJ, Markham A. Finasteride: A review of its use in Male Pattern Hair Loss. Drugs (1999) 57, 111–126.
30. Fabbrocinic H, Cantelli M, Masara A, Annuziata Mc, Marasca C, Cacciapuoti S. Female Pattern hair loss: A clinical Pathophysiologic and Therapeutic Revie. International Journal of Women’s dermatology 2018; 4(4): 203-211.
31. Pirmohamed, M. (2014). Personalized pharmacogenomics: predicting efficacy and adverse drug reactions. Annual review of genomics and human genetics, 15, 349-370.