CLINICAL
Pillar to post
Mr Arturo Almeida concludes his two-part series on the lower face with his three-pillar approach to rejuvenation
MR ARTURO ALMEIDA
Mr Arturo Almeida is an internationally-renowned keynote speaker, medical trainer and expert in minimally-invasive and non-surgical cosmetic procedures. A consultant surgeon, he has been practicing cosmetic medicine for more than 13 years. He is a Medical Ambassador of International Plastic Aesthetic Residence (IPAR) and is based in Leeds, practicing at the VSL Clinic in Wakefield and Blemish Clinic in Manchester.
In last month’s issue of Aesthetic Medicine, I explored the ageing and anatomy of the lower face. This month I will discuss the treatment options available to us and will introduce my three-pillar approach to rejuvenation of the lower third, encompassing volume and bone restoration, improvement of skin sagginess and the dissolving of submental fat.
THE THREE-PILLAR APPROACH
I base my lower face contouring on three pillars:
• Volume and bone restoration
• Improvement of skin sagginess
• Dissolving of submental fat
Volume and bone restoration
Volume and bone restoration is the first pillar of my approach. If you don’t restore the volume and bone mass lost through the ageing process you probably won’t achieve good results with your lower face treatments. You can treat the tip of the iceberg doing other things but, unless you tackle what is happening underneath you won’t be successful and your patients won’t be happy.

Figure 1: The three boluses underneath the mentalis muscle supraperiosteal
When considering volume and bone restoration, there are three important landmarks: the chin, the angle of the mandible and the pre-jowl sulcus. For the chin, my preference is to use a premium dermal filler with a high G prime, which is great to restore volume at the bone level. The availability of such fillers has changed the way I approach lower face rejuvenation.
Although we are all familiar with Allergan’s Voluma and Volux, in my practice I normally use Sinclair’s Perfectha Subskin. It is a great filler that produces great volumisation. The other product that I use – and this is just my personal preference – is Teoxane’s Teosyal RHA 4.
The technique I recommend is to pinch the chin with two fingers, using your nondominant hand, and then to inject one to three boluses underneath the mentalis muscle supraperiosteal (figure 1), aspirating first before injecting. Despite the controversy over whether or not aspiration is accurate, I think it is a safety measure that we should always take when doing boluses, particularly deep boluses.
I normally inject 0.2ml, sometimes 0.3ml, per point, but never use more than 1ml in total. Recently, some publications have reported an increased bone resorption due to excess dermal filler in the mentonian area, so we have to be careful with the total amount of filler delivered. Sometimes we need to treat the mentolabial sulcus itself, so if that is the case, I normally I inject 0.2ml from each side.
I use a 25G blunt cannula to inject the mentolabial sulcus. For the chin, my personal preference is a needle. My belief is that you should use the tools you feel confident with, and not exclusively a cannula or needle.

Figure 2
The next important point is the angle of the mandible and for that I use a deep bolus, normally 0.2 to 0.25ml, of a high G prime filler.
You can inject point one (see figure 2) with a cannula or you can go perpendicular to the angle; both approaches will work. When I go perpendicular I use a needle, again aspirating carefully before injecting slowly. As we all have the fear of causing a possible vascular occlusion, pay attention to what you are doing and don’t get distracted. This is of key importance, not just for the lower face, but for any treatments we deliver to our patients.
The next point is the pre-jowl sulcus. Again, I use another deep bolus – 0.15 to 0.2ml – and from here, I like to use a fanning technique to treat the entire mandible (figure 2). For this, I do use a cannula, because as the facial artery runs through this area, you don’t want to hit the artery with a needle.

Figure 3: Before and after three-point injections
CASE STUDY
Let me share with you a case that I recently treated. This patient was 49 years old and wanted to get ready for her 50th birthday.
Her chin was good but it needed a little bit of anterior projection. However, the main thing that was bothering her was the jowling she had started to see.
The technique that I used was to inject single boluses of filler at three points. At the most anterior injection point I used 0.25ml and then I did another bonus injection of 0.2ml at the gonial angle.
The last bolus was at the pre-jowl sulcus with no additional fanning and three injections on each side. As you can see in figure 3, her chin was slightly more projected, the jowls are no longer present because we gave the support at the pre-jowl sulcus, and the lower mandible is now well defined.
Improve skin sagginess
Second, we need to improve the sagginess and appearance of the skin. For skin sagginess we can again use dermal fillers and also threads, which are becoming more and more popular.
For the skin’s appearance I normally choose TCA-based chemical peels, which are great for improving skin quality. My preference is Easy TCA by Skin Tech Pharma Group. When properly done they provide a nice revitalisation of the area and produce skin tightening thanks to the stimulation of collagen production that occurs after a good medium depth chemical peel.
Dissolve submental fat pockets
The last pillar of my approach to lower face contouring is the treatment of the submental fat pockets, AKA the double chin. For this purpose, I use fat-dissolving injections.
It’s true that are other methods to tackle this problem, including tumescent liposuction surgery and devices with specially-designed handpieces that are suitable to treat the submental fat area.
But I have used fat-dissolving injectables since 2008 and have been training medical practitioners in these treatments since 2011. I am aware that some practitioners feel these injections are not suitable for all patients and could even be dangerous. It is also a fact that UK insurers charge a premium and an excess to cover these treatments, which is not the case in other countries.
However, in my experience and in that of many others, these agents are very safe to use and with low incidence of side effects, assuming the proper technique is used.
The active principle is deoxycholic acid (DCA), a naturally-occurring secondary bile acid. DCA acts by rupturing the cell membrane of the adipocyte, breaking down the cell and releasing its contents, including the vacuole containing the fat. Therefore, an actual destruction of the fat tissue occurs, a process known as adipocytolysis, which is different from lipolysis, a biological process that breaks down the fat within the adipocyte.
When injury occurs in our body – as is the case with adipocitolysis – the normal response is an inflammatory reaction. So, swelling will always occur after these treatments, mainly when treating the double chin.
However, I always tell my patients that swelling should be seen as a positive sign as it means we have achieved some degree of fat tissue destruction. The next stage in this process (figure 4) is remodelling, where collagen is produced, and some degree of skin tightening occurs. The final stage, resolution, is when volume reduction is achieved.
Among the agents currently available in the UK to treat the double chin, my choice is
Celluform+ from Promoitalia SLP, as it has a unique formulation specifically designed for submental fat that produces really good results with less swelling compared to other agents. Allergan’s Belkyra – the only FDAapproved fat dissolving agent – is not yet available in the UK market.
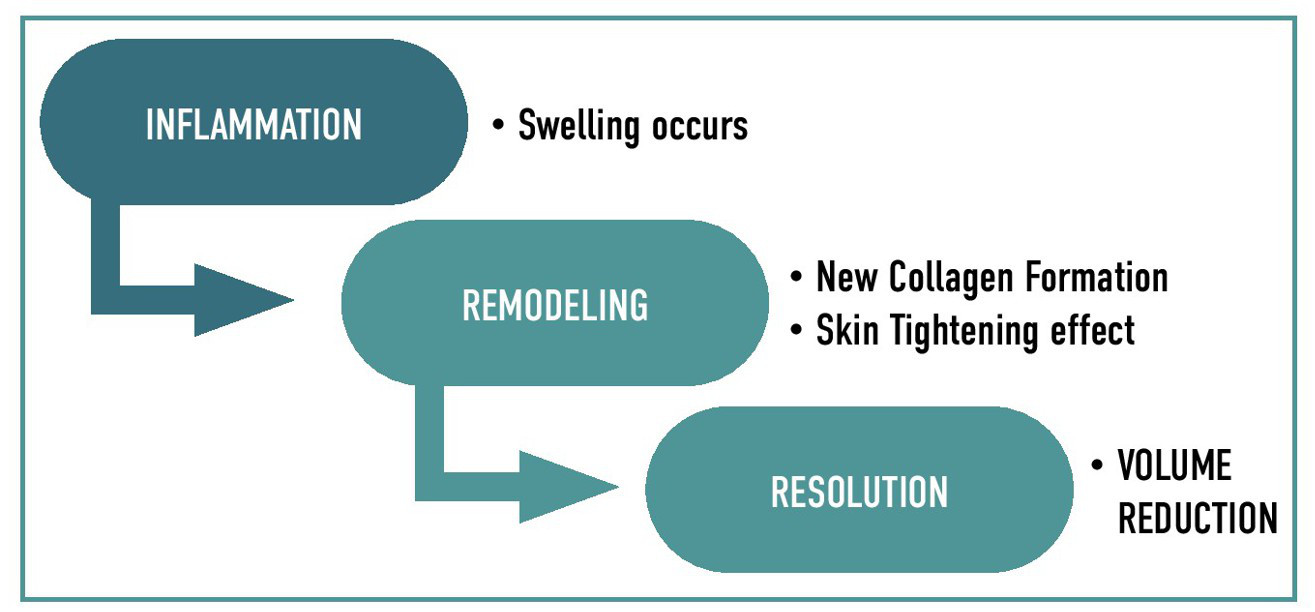
Figure 4: The body’s inflammatory response to fat-dissolving injections
CASE STUDY
To finish, I will share another of my cases. This patient had always been annoyed by her double chin.I treated her exclusively with 3ml of Celluform+ (figure 5).
Six weeks after the procedure, I saw her for a follow-up. Although there is not much change in volume, her face profile is now slimmer and the skin-tightening effect has created the improvement in the cervicomental angle, so it served as a perfect lower-face contouring treatment. The patient was delighted because, in her opinion, the shape of her lower face had improved massively.
This case speaks for itself, and I think fatdissolving injections are a must-have in your toolbox for lower face rejuvenation.

Figure 5: Before and after Celluform+