HAIR LOSS
Hair loss and medication
Losing hair can be a very traumatic event. Dr Nilofer Farjo, hair restoration surgeon and founding director of the Farjo Hair Institute, looks at how certain medications can impact hair growth.
The most common cause of hair loss is genetic susceptibility but there are quite a few other things that can cause hair to fall out either temporarily or permanently. Sometimes it is the skin that has a condition which then affects the hair but often it is something that affects how the hair grows either from a medical condition or an external source. The normal life cycle of hair is a growth or anagen phase lasting three to four years followed by a short period of transition (catagen phase) leading to the resting phase (telogen) which normally lasts three to four months.
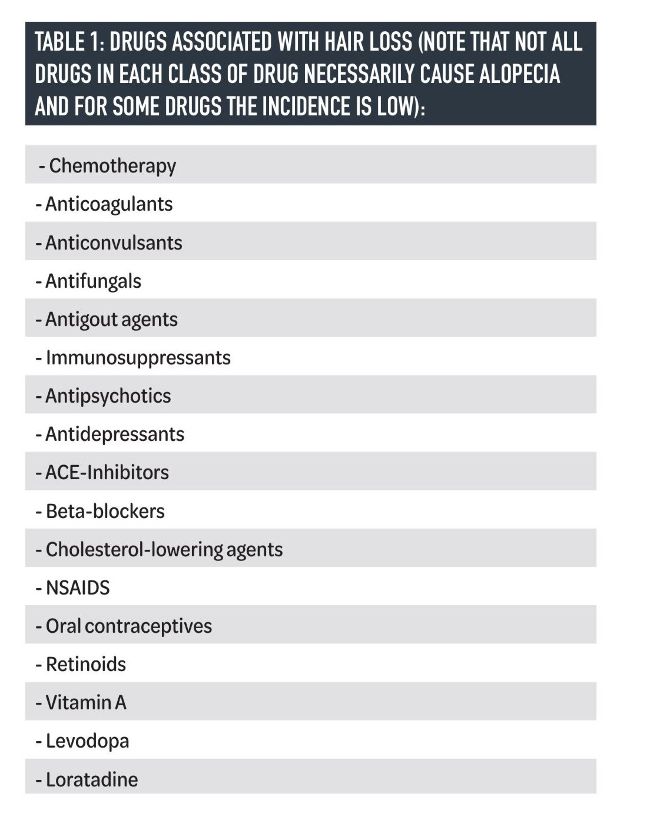
It is worth knowing that many things can impact the hair’s growth cycle, including some medications (table 1). Side effects often subside when medication is stopped, but that doesn’t make the experience any less inconvenient or distressing. It’s important to be aware of all the side effects of medications beforehand but patients should never stop a medication without discussing it with their specialist as that can be harmful to their health. In this article, we explore the most common medications which can affect hair growth.
CANCER DRUGS:
The most obvious drugs that we think about with regard to hair loss are anticancer drugs. However, not all cancer drugs will cause hair loss, and some will cause diffuse thinning rather than complete hair loss. It is important to tell patients to ask about the side effects of their medications and if it causes hair loss what they can do. For example, cold therapy just before giving chemotherapy is now being offered in some centres on the NHS. Although it is an uncomfortable experience to wear a cooling cap1most patients are happy with the outcome. And it’s not just the scalp hair that goes but all the hair on the body. It is surprising to learn that about 10% of patients say they would rather take their chances with cancer than experience hair loss, but I would not advise this approach.
A discussion beforehand with a patient on the options such as cutting hair shorter in the build-up to chemo, matching wig colour and style to their hair beforehand, asking their specialist about the cold cap, asking about recovery time, etc. would be sensible. It is also important to let people know that they can learn to pencil in or get tattooing of their eyebrows with semipermanent makeup and again do this while they still have their eyebrows so they can get the right shape and colour. Artificial eyelashes may also be an option, but they must check first as some chemo agents cause dry eyes and skin problems.2
A discussion about hair re-growth is also worthwhile as abnormal/dystrophic growth can occur in which hair texture (wiry or kinky) and colour (darkening or pigmentation) can be different at least for the first hair growth cycle of three to four years. Sometimes, hair loss is permanent or there can be partial re-growth. But this can only be confirmed about 18 months or longer after stopping the chemotherapy.
ORAL CONTRACEPTIVES AND HRT:
Oral contraceptives and hormone replacement therapy can affect hair by influencing and altering the body’s natural hormone levels, resulting in potential thinning and slower growth. The progesterone in these drugs can trigger hair loss if they have a high androgen index i.e. they behave similarly to male hormones.3As previously mentioned, genetic susceptibility to balding is inherited but you also need male hormones and that’s why people don’t experience hair loss before puberty. In men, testosterone (an androgen) converts to dihydrotestosterone in the body which can attach to hair follicle receptors and change the growth cycle if they have the genetics for hair loss. Therefore, the medical term for balding is androgenetic alopecia (male hormone + genetics causes hair loss).
Women have much less testosterone so never go as bald as men; however, the progesterone in their body can convert to androgens which will then accelerate hair loss. So, if they take hormones and get more androgenic effects such as acne and hair loss the type of progesterone in the pill may be causing these effects. In that case, they can ask their doctor to change to a different contraceptive or HRT.
EPILEPSY MEDICATION:
Epilepsy drugs have been shown to cause some hair loss and possibly make hair curlier. Valproic acid (VPA) which is also referred to as sodium valproate is the first-line treatment for epilepsy and is also used to treat migraines, bipolar disorder, and nerve pain. Amongst epilepsy drugs, VPA has the highest incidence of hair loss at 11% compared to 0.3-1% for other drugs.4This usually occurs within six months of commencing the drug. As for chemotherapy drugs, hair growth can be abnormal, resulting in kinking or curling of the hair fibres, as well as pigment cells being activated causing hair to becomes darker.
ANTI-COAGULANTS/BLOOD THINNERS:
There are several drugs in this group such as heparins and coumarins (e.g. warfarin) which can potentially cause hair loss. Newer drugs have also been reported to cause hair thinning as an adverse effect but to a lesser degree. The type of hair loss tends to be very diffuse and is caused by anagen hairs being pushed into the resting phase.
The shedding that occurs takes time and may not be apparent for several months, if at all, and therefore may be under-reported. Variability in the normal daily hair shedding (average 100 hairs/ day) means that slight increases don’t cause cosmetically visible alopecia. There are a few case studies which report sudden and severe hair loss which may be the reason why the exact mechanism causing the shedding is unclear. In some of these cases changing to a different anti-coagulant solved the problem but, in all cases, when the drug was stopped hair returned to normal.5If a patient experiences hair loss they should be referred to their prescribing doctor.
ACNE MEDICATION:
Isotretinoin (brand name Retin-A, Accutane, etc) is a drug that is used to treat severe acne by reducing sebum production and sebaceous glands. However, it can have some serious side effects such as kidney and liver problems which means it must be monitored carefully by the prescribing doctor. Less commonly it causes hair loss which is diffuse and caused by anagen hairs being pushed into the resting phase with telogen effluvium occurring about three months after starting therapy. There may therefore be a change in the density of hair. The amount of hair loss is dose-dependent, but the incidence is low in all cases. Patients on <0.5 mg/kg/d of isotretinoin experienced hair loss at a frequency of 3.2% (n = 18/565) compared with those on ≥0.5 mg/kg/d, who experienced hair loss at a frequency of 5.7% (n = 192/3375).6
PSORIASIS MEDICATION:
Psoriasis itself can cause hair loss in some patients either due to inflammation or due to rubbing or picking of the skin plaques. When the condition is treated and inflammation subsides, hair usually grows back. However, there are a small number of patients in which the hair follicle can be destroyed, and scarring alopecia occurs.7It is also well known that methotrexate (an immune system modulator and chemotherapy agent) which is a common drug used to treat psoriasis causes hair loss in 5-10% of patients. It does this by decreasing cell turnover so slowing the rate of hair growth.
CONCLUSION:
Many drugs cause hair loss but usually in a minority of people. Before treating a patient, a full medical history including medications is important. The main ones to consider as a practitioner are chemotherapy, immune modulators, and hormones. The aesthetic practitioner is particularly helpful for patients who will be starting chemotherapy as some very practical things are useful. For other medications, ifyou suspect that they are causing hair loss then the patient should be referred to their GP or specialist to see if their medications can either be reduced in dose or changed to an alternative. If the patient can’t change their medication or they have permanent hair loss then a dermatology referral may be warranted or in straightforward cases, the patient may be helped by minoxidil.
REFERENCES
1. https://www.macmillan.org.uk/cancer-information-and-support/impacts-of-cancer/hair-loss/scalp-cooling
2. https://www.nhs.uk/conditions/chemotherapy/cancer-and-hair-loss/
3. Alopecia due to high androgen index contraceptive. Graves, Katelyn Y. PhD; Smith, Benjamin J. PA-C, DFAAPA; Nuccio, Brigitta C. Journal Am Acad Physician Assistants. August 2018 Vol 31:8, 20-24
4. Risk of valproic acid-related alopecia:A systematic review and meta-analysis. Wang X, Wang H,Xu D, Zhu L, Liu L. Seizure: European Journal of Epilepsy 69 (2019) 61-69.
5. Traditional Anticoagulants and Hair Loss: A Role for Direct Oral Anticoagulants? A Review of the Literature. Watras MM, PatelJP,Arya R. Drugs Real World Outcomes 2016 Mar; 3(1): 1–6.
6. Comparing the frequency of isotretinoin-induced hair loss at <0.5-mg/kg/d versus ≥0.5-mg/kg/d dosing in acne patients: A systematic review. Lytvyn Y, McDonald K, Mufti A, BeeckerJ.JAAD Int. 2022 Feb 10;6:125-142
7. Psoriatic Alopecia. George SMC, Taylor MR, Farrant PBJ. Clin Exp Derm 2015 Oct; 40(7):717-21